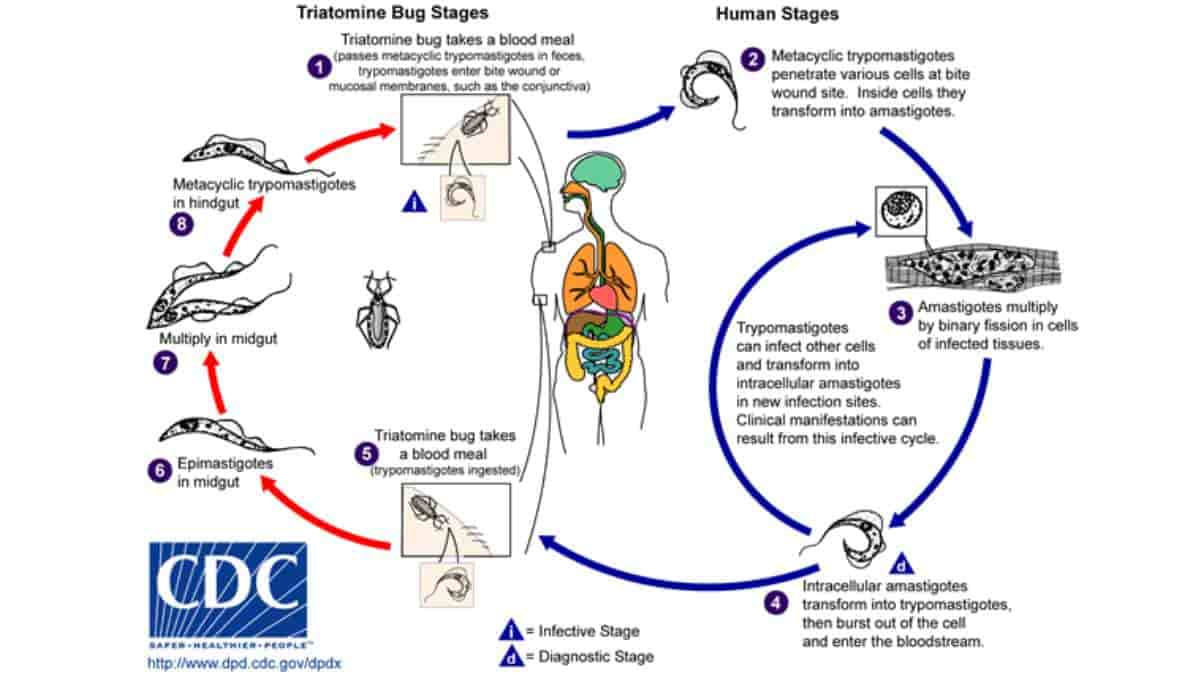
American trypanosomiasis is also known as Chagas disease. It is the human tropical parasitic disease that occurs mainly in South America. The flagellate protozoan named Trypanosoma cruzi is the cause of the transmission to humans from other mammals mostly by the blood-sucking assassin bugs.
These assassin bugs are known by other names such as the kissing bug, chipo, chupanca, benchuca, barbeiro and vinchuca. There are other ways to get the disease including by ingestion of contaminated food, blood transfusion and fetal-maternal transmission.
The bed bug may be equally as dangerous as its evil cousin, the triatomine, or “kissing” bug. A 2014 study from Penn Medicine’s Center for Clinical Epidemiology and Biostatistics found that bed bugs, like triatomines, can spread Trypanosoma cruzi, the parasite that causes Chagas disease.
Bed bugs and kissing bugs are distant cousins but share many striking similarities. Both insects hide in household cracks and crevices waiting for nightfall and the opportunity to feed on sleeping hosts. They are from the same order of insects (Hemiptera) and both only feed on blood. (One main difference is their size: kissing bugs are five times as big as a bed bug).
Chagas’ disease has affected approximately 18 million people and kills and estimated 50,000 people yearly. It is a big problem in Latin America and in the United States where approximately 500,000 individuals are infected who have emigrated there from Latin American countries. In Latin America it is mostly concentrated in the rural areas of Central and South America.
There are two stages to the disease: the acute stage and the chronic stage. The acute stage is the first stage and the chronic stage develops over the next 10 years.
Acute Stage:
A local skin nodule (chagoma) appears at the site of the bite. The individual will develop conjunctival mucous membranes or unilateral periorbital edema or preauricular lymphadenitis. The combined symptoms are called: Roma’s sign.
Fever, anorexia, lymphadenopathy, and mild hepatosplenomegaly or myocarditis may occur. Approximately 20% of acute cases can resolve over 2 to 3 months only to reappear after several years.
The Chronic Stage:
This stage won’t appear until years even decades after the initial infection. The nervous system, digestive system and the heart can be affected in this stage. Dementia, cardiomyopathy and digestive tract disorders (megacolon and megaesophagus) may occur and also weight loss.
Some patients may experience difficulty swallowing which may lead to malnutrition. 27% of patients develop cardiac problems, 6% develop digestive damage and 3% develop nervous system involvement. If not treated Chagas can be fatal, usually due to cardiomyopathy.
Treatment:
Drugs are only effective if they are given to the patient during the acute phase. The drugs of choice are azole or nitroderivatives or nifurtimox. These drugs have adverse side effects.
In the chronic stage the symptoms are treated such as cardiac failure being treated by a heart pacemaker and surgery for megaintestine. The disease is not curable once it reaches the chronic stage.
Prevention:
In the 70s a vaccine was developed using cellular and subcellular fractions of the parasite (kissing bug) but it was not economically feasible. There is current research being conducted to test potential DNA vaccines.
As most tropical diseases prevention centers on ridding the community of the vector causing the disease in this case the kissing bug
Communities use sprays and paints that contain insecticides to help decrease the bug population. Improving sanitation and housing conditions in rural areas can also help. The use of a mosquito net is required. In most countries where Chagas’ disease is endemic, there is already mandatory blood testing before a blood donation can be accepted.
As with any of the tropical diseases, research and education are key components to controlling the disease.
References:
- Bern C (July 2015). Chagas’ disease. N. Engl. J. Med. (Review). 373 (5): 456–66. doi:10.1056/NEJMra1410150
- Bern C, Messenger LA, Whitman JD, Maguire JH (2019). Chagas Disease in the United States: a Public Health Approach. Clinical Microbiology Reviews (Review). 33 (1). doi:10.1128/CMR.00023-19
- Capinera JL, ed. (2008). Encyclopedia of entomology (2nd ed.). Dordrecht: Springer. ISBN 9781402062421
- Despommier DD, Griffin DO, Gwadz RW, Hotez PJ, Knirsch CA (2019). American Trypanosomiasis, in Parasitic Diseases (7 ed.). New York: Parasites Without Borders
- Pérez-Molina JA, Molina I (2018). Chagas disease. The Lancet. 391 (10115): 82–94. doi:10.1016/S0140-6736(17)31612-4
- Renzo Salazar, Ricardo Castillo-Neyra, Aaron W. Tustin, Katty Borrini-Mayorí, César Náquira, and Michael Z. Levy. Original Article: Bed Bugs (Cimex lectularius) as Vectors of Trypanosoma cruzi. American Journal of Tropical Medicine and Hygiene, November 2014 DOI: 10.4269/ajtmh.14-0483
Last Updated on April 8, 2024